Total Items
0
0 Item(s)


Blog post
Comparison of the Effectiveness of Traditional Motorized Traction and Non-surgical Spinal Decompression Therapy Added to Conventional Physiotherapy for Treatment of Chronic Low Back PainSevda Adar, Onurhan Apaydın, Umit Dündar, Hasan Toktas, Hilal Yesil, Selma Eroglu, Nuran Eyvaz Originally published: Cureus 16(9): e69610. doi:10.7759/cureus.69610, September 14, 2024 Background: There are a limited number of studies comparing traditional motorized traction and non-surgical spinal decompression with other treatment options such as conventional motor traction in the treatment of low back pain caused by lumbar discopathy. This retrospective study aimed to compare the effectiveness of these treatments. Methods: The retrospective data of patients diagnosed with lumbar discopathy who underwent physical therapy in our clinic were reviewed. Demographic data, duration of their symptoms, physical examination findings, lumbosacral magnetic resonance imaging (MRI) reports, method and duration of treatment, and visual analog scale (VAS) and Oswestry Disability Index (ODI) results were recorded. Results: A total of 160 patients met the inclusion criteria. Their mean age was 44.6±12.4 (range 21-65) years, 57.5% (n=92) were female, and 42.5% (n=68) were male. There were no differences between the conventional physiotherapy, motorized traction, and spinal decompression groups in terms of age, duration of symptoms, and the number of sessions (p>0.05). In all three groups, the mean scores of VAS and ODI were significantly decreased in the pre-and post-treatment comparisons (p<0.005). The rates of change in VAS and ODI were higher in the traction group and spinal decompression group compared to the conventional treatment (p<0.005). Conclusion: In patients with subacute and chronic lumbar discopathies, motorized traction and spinal decompression treatments added to conventional treatment were found to be more effective than conventional treatment alone. The results of spinal decompression and conventional motorized traction treatments appear to be similar. Image Copyright © 2024, Adar et al. Patients who received motorized traction treatment with the Chattanooga Triton Traction Machine 4798 for three days a week in addition to conventional physiotherapy were included in the Motorized Traction Group. References: Burden of chronic low back pain: Association with pain severity and prescription medication use in five large European countries. Perrot S, Doane MJ, Jaffe DH, et al. Pain Pract. 2022;22:359–371. - PMC - PubMed What low back pain is and why we need to pay attention. Hartvigsen J, Hancock MJ, Kongsted A, et al. Lancet. 2018;391:2356–2367. - PubMed Clinical efficacy of mechanical traction as physical therapy for lumbar disc herniation: a meta-analysis. Wang W, Long F, Wu X, Li S, Lin J. Comput Math Methods Med. 2022;2022:5670303. - PMC - PubMed Nonsurgical treatments for patients with radicular pain from lumbosacral disc herniation. Lee JH, Choi KH, Kang S, et al. Spine J. 2019;19:1478–1489. - PubMed Effectiveness of mechanical traction for lumbar radiculopathy: A systematic review and meta-analysis. Vanti C, Panizzolo A, Turone L, Guccione AA, Violante FS, Pillastrini P, Bertozzi L. Phys Ther. 2021;101:0. - PubMed

Blog post
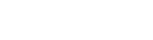
A Controlled Randomized Trial with a 12-week Follow-Up Investigating the Effects of Medium-Frequency Neuromuscular Electrical Stimulation on Pain, VMO Thickness, and Functionality in Patients with Knee OsteoarthritisAzar Moezy, Soheila Masoudi, Ahmad Nazari, Arezoo Abasi PurposeThis study was conducted to assess the effectiveness of neuromuscular electrical stimulation (NMES) and exercise therapy (Exs) in improving pain, muscle weakness, and function in patients with knee osteoarthritis (KOA). Methods: Participants: 75 female patients with mild-to-moderate KOA. Treatment: Participants were randomly assigned to one of three groups: NMES Only: Pre-Modulated Interferential two-pole currents were used. The proximal electrode was aligned with the Rectus Femoris and the distal electrode was placed over the vastus medialis oblique. Treatment parameters consisted of the following: Pulse Width: 600μs Carrier Frequencies: 4,000—4,050 Hz Beat Frequency: 50 Hz Duration: 15 minutes Current Intensity: Adjusted for effective muscle contractions while avoiding pain or discomfort Exs Only: Completed 5 exercises including quad contractions, straight leg raises, knee extensions, hip adductor contractions, and a wall-sit. NMES + Exs: Participants in this group completed both NMES and exercises as described above. Participants completed 12 treatment sessions over 4 weeks. Prior to treatment, all participants received 20 minutes of transcutaneous electrical nerve stimulation for pain management. Participants were also instructed to not take non-steroidal anti-inflammatory drugs during the treatment period. A daily maximum of 2 g of acetaminophen was allowed if patients had pain. Assessments: Study outcome measures included the Visual Analog Scale (VAS), knee flexion range of motion (FROM), thigh muscle girth (TG), VMO thickness, timed up and go test (TUG), six-minute walk test (6MWT), and WOMAC scores. Outcome measures were assessed at baseline, post-treatment, and at 12 weeks follow-up. Results Pain Reduction: The VAS scores in all 3 groups significantly improved post-treatment and at the 12 week follow-up. At the 12 week follow-up, the NMES Only group had the greatest reduction in pain compared to the other 2 groups. Functional Improvements: All 3 groups significantly improved post-treatment and at the 12 week follow-up in 6MWT, TUG, and WOMAC scores. The NMES Only and NMES + Exs groups also had significant improvement in VMO thickness and FROM. NMES Only: The NMES only group improved the most in the 6MWT and TUG tests compared to the other groups post-intervention and at the 12 week follow-up and had the best total WOMAC score at the 12 week follow-up. NMES + Exs: The group that received NMES along with exercise had better outcomes than the other groups in FROM, TG, and VMO thickness post-intervention and at follow-up. This group also achieved better WOMAC stiffness scores post-intervention and at follow-up compared to the other 2 groups. Conclusion NMES is an effective treatment option for improving pain and physical function in KOA patients. Combining NMES with exercise is also an effective method of managing KOA as demonstrated by the enhanced FROM, increased muscle thickness, and improved WOMAC stiffness scores.

Blog post
High-Intensity Laser Therapy vs Red Light Therapy: What's the Difference?High-intensity laser therapy (HILT) and LED-based red light therapy (RLT) are often grouped together under the umbrella of light-based therapy, known as photobiomodulation therapy (PBMT). While they both fall within this broader category of photobiomodulation (PBM), they are not interchangeable. HILT and RLT represent distinct approaches with different clinical capabilities and therapeutic outcomes. PBM refers to the use of specific wavelengths of light both in the visible and near-infrared spectrum to influence cellular function, promote tissue repair, and alleviate pain. Both high-powered lasers and low-powered LEDs can be used to deliver PBMT, including red light wavelengths, but the differences in light source and energy output are clinically significant. Red Light Therapy (RLT) utilizes low-power LEDs that emit non-coherent light, making it suitable for surface-level applications such as skin care, hair growth, and general wellness. RLT LEDs are commonly organized in arrays of multiple LEDs and sold as panels, masks, and hats. High-Intensity Laser Therapy (HILT) employs Class IV medical lasers that deliver coherent, high-powered near-infrared light capable of penetrating deep into soft tissue, joints, and muscles. This allows for more targeted treatment of musculoskeletal conditions. Some HILT devices include a red light wavelength at higher powers than RLT LEDs. In the sections that follow, we'll explore how these therapies differ in terms of clinical application, treatment outcomes, and why HILT is the preferred choice for deeper, targeted interventions. Here’s What You Really Need to Know High-intensity laser therapy (HILT) uses targeted near-infrared laser light to deliver therapeutic energy deep into soft tissues, joints, and muscles. In contrast, red light therapy (RLT) typically uses low-powered LEDs that produce broader, more superficial effects. Laser therapy is widely used in clinical settings to support musculoskeletal conditions, while red light therapy is more commonly found in wellness centers and at-home devices. What Is High-Intensity Laser Therapy? HILT uses Class IV medical lasers, like those developed by LightForce®, to influence cellular activity, promote circulation, and support the body’s natural recovery processes. LightForce® devices use near-infrared wavelengths (810nm, 980nm), which can penetrate deeply—up to several centimeters—into soft tissue. This makes them ideal for applications involving pain, muscle spasm, and joint stiffness. Image What Is Red Light Therapy? Red light therapy is a lower-powered form of PBMT that uses LEDs to emit red light (625-750 nm). These treatments are commonly marketed for cosmetic or wellness purposes. While RLT may offer benefits such as improved skin health, hair growth, and pain relief, it lacks the power and tissue penetration necessary to impact deeper musculoskeletal structures. It is not generally designed for clinical use. HILT vs RLT: Quick Summary Feature High-Intensity Laser Therapy (HILT) Red Light Therapy (RLT) Light Source High-power Class IV laser Low-power LED Penetration Depth Up to 12 cm Up to 0.5 cm Clinical Use Medical and rehabilitation settings Home, spa, wellness Power Output 500mW – 40W (LightForce® XLi) 10 – 500mW Primary Purpose Pain relief, recovery Skin, hair growth, general wellness Treatment Duration Usually 2–10 minutes, depending on the treatment area 10–30+ minutes Results Timeline Often noticeable after 1–3 sessions May take weeks Why Laser Therapy Is Better for Deep Tissue Conditions While both therapies use light to stimulation biological responses, laser therapy offers several clinical advantages: Reaches deeper into soft tissue, joints, and muscle Provides a controlled and concentrated dose of energy Can achieve meaningful outcomes with fewer visits This is why high-intensity laser therapy is commonly used in: Sports medicine and recovery Arthritis and joint discomfort Acute and chronic soft tissue support Why Choose LightForce® Lasers? At LightForce®, we specialize in high-intensity laser therapy—backed by science and trusted by professionals. Our Class IV medical lasers are used by: Elite athletic trainers and professional sports teams Physical therapists and chiropractors Pain management physicians and rehabilitation clinics LightForce® Therapy Lasers are known around the world for innovative technology and evidence-based treatment solutions. With thousands of customers across the globe, Chattanooga® estimates over 1 million+ treatments are performed using LightForce® Therapy Lasers per month. LightForce® Therapy Lasers are unique among laser devices in having a singular focus in rehabilitation and pain management. Over 250 professional and college sports teams trust LightForce® Therapy Lasers for their athletes.¹ Take the Next Steps Toward Real Relief If you’re looking for results beyond what over-the-counter wellness tools can offer, it’s time to explore the advantages of high-intensity laser therapy with LightForce®. Schedule a demonstration with your local territory manager today. References: ¹ Figure based on LightForce® customers in the professional, college, and Olympic sports industries.

Blog post
Learn and Earn CEUs with Your Chattanooga ModalitiesIn partnership with Torrentia, a clinician-led education company, we are thrilled to offer Chattanooga® customers and friends a way to earn CEU credits while learning how to more effectively integrate your existing modalities, improve patient outcomes, and expand your clinic services. The Orthobiological Hacker™ (OBH) Certification gives licensed rehab professionals hands-on experience combining technologies like high-intensity laser, shockwave, NMES, and orthobiologics with step-by-step protocols. You will leave with actionable strategies and access to a network of clinicians advancing regenerative rehabilitation. What Is It? The OBH Certification is designed for clinicians who want to use advanced modalities more confidently in daily practice. Through live intensive sessions and digital coursework, you will: Earn up to 33 CEU credits Integrate your laser, shockwave, and orthobiologic tools more effectively Apply advanced techniques to help improve patient outcomes Expand cash-based and hybrid service offerings Train your team to implement new protocols Who is Torrentia? Torrentia is a clinician-led education company dedicated to helping rehabilitation professionals integrate advanced modalities like high-intensity laser and shockwave into their practice. What They Do: Torrentia delivers certification programs for physical therapists, chiropractors, athletic trainers, and other rehab-focused clinicians who are looking to adopt advanced tools and protocols. The Orthobiological Hacker™ Certification helps teach clinicians how to integrate technologies like high-intensity laser, shockwave therapy, and dry needling. Torrentia combines hands-on lab training, live intensives, and digital modules. Participants can earn up to 33 CEU credits and access ongoing mentorship and a community of peers. Why It Matters: In the evolving world of rehabilitation and regenerative care, success requires more than purchasing new technology—it requires frameworks, training, and systems for effective application. Torrentia helps clinicians by: Bridging the gap between rehab methods and emerging tools, helping clinicians confidently adopt new technologies. Focusing on practical implementation, including dosing, staging of interventions, team training, referral integration, and business strategy. Supporting cash-based service models, helping practices grow their revenue and clinical impact. Torrentia offers ongoing certification sessions throughout the US. Find your next session here: Register

Blog post
Comparison Between Low-Level and High-Intensity Laser Therapy as an Adjunctive Treatment for Knee Osteoarthritis: A Randomized, Double-Blind Clinical TrialAhmad MA, Moganan M, A Hamid MS, Sulaiman N, Moorthy U, Hasnan N, Yusof A. Purpose: This study was conducted to determine whether high-intensity laser therapy (HILT) or low-level laser therapy (LLLT) provides better pain and functional outcomes for patients with knee osteoarthritis (KOA) when used as an adjunct to exercise therapy (EX). Methods: Participants: 34 adults with mild-to-moderate KOA. Treatment: All participants completed an exercise program tailored to the individual’s needs and was conducted weekly for 12 weeks. Participants were randomly assigned to either: HILT + EX: Patients in this group were treated with laser therapy once per week for 15 minutes for 12 weeks. The laser had an output power of 5 W, and patients received a total dose of 3,190 J per session. LLLT + EX: Patients in this group were treated with laser therapy once per week for 15 minutes for 12 weeks. The laser had a peak output power of 400 mW, and patients received a total dose of 400 J per session. Assessments: Study outcome measures included the Knee Injury and Osteoarthritis Outcome Score (KOOS), Numerical Pain Rating Scale (NPRS), active knee flexion, and Timed Up-and-Go test (TUG). Outcomes were assessed prior to start of laser therapy and after 12 weeks of treatment. Results: Improvements: Though both groups showed statistically significant improvements in KOOS, NPRS, active knee flexion, and TUG scores compared to baseline, the HILT + EX group performed significantly better in all outcomes. The HILT + EX group also demonstrated clinically significant improvement in KOOS and NPRS. HILT vs. LLLT: HILT is better than LLLT in relieving KOA patients’ pain and improving their physical function and knee-related quality of life. For example, the average LLLT + EX group pain score decreased by 32%, but the average HILT + EX group pain score decreased by 50%. In addition, the average KOOS score for the HILT + EX group improved by 32% while the LLLT + EX group improved by only 11%. Conclusion: Effectiveness: Combining laser therapy with knee rehabilitation exercises improves KOA patients’ knee pain, function, and mobility. Because the best results were seen when patients were treated with a high-intensity laser, the authors suggest that HILT is the more effective treatment option than LLLT for managing KOA. Citation: Ahmad MA, Moganan M, A Hamid MS, et al. Comparison between Low-Level and High-Intensity Laser Therapy as an Adjunctive Treatment for Knee Osteoarthritis: A Randomized, Double-Blind Clinical Trial. Life (Basel). 2023;13(7):1519. Published 2023 Jul 6. doi:10.3390/life13071519
Blog post
Effects of Neuromuscular Electrical Stimulation on Quadriceps Femoris Muscle Strength and Knee Joint Function in Patients After ACL Surgery: A Systematic Review and Meta-analysis of Randomized Controlled TrialsZhikuan Li, Lingpeng Jin, Zhen Chen, Ziqi Shang, Yue Geng, Siman Tian, Jiangtao Dong Purpose: This systematic review and meta-analysis was conducted to investigate the effects of neuromuscular electrical stimulation (NMES) on quadriceps strength and knee function after anterior cruciate ligament (ACL) surgery. Methods: Study Selection: Included randomized controlled trials where NMES was part of the ACL surgery postoperative rehabilitation protocol and compared to standard physical therapy as the control group. Eleven studies met the inclusion criteria (N = 202 patients receiving NMES; N = 200 patients in control group). Assessments: Quadriceps strength was measured using isometric or isokinetic tests. Knee function was assessed using the Lysholm score. Results: Meta-analysis analysis – Knee Function: Three studies were included in the meta-analysis to assess knee function using the Lysholm score. This analysis revealed no statistical difference in knee function between the NMES and control groups. However, there was a medium to high degree of heterogeneity. Other knee function assessments used in the studies, including the International Knee Documentation Committee, Knee Injury and Osteoarthritis Outcome Score-Activities of Daily Living, and the Knee Outcome Survey-Activities of Daily Living Scale did show some positive effect of NMES on knee function. Meta-analysis – Muscle Strength: Nine studies were included in the meta-analysis to assess muscle strength. The analysis demonstrated that NMES combined with standard physical therapy significantly improves quadriceps strength when compared to physical therapy alone at both short (≤ 6 weeks) and long-term (> 6 week) follow-up. Subgroup analysis –Timing of NMES: This analysis showed that starting physical rehabilitation with NMES earlier in the post-operative course (≤ 1 week post-surgery) resulted in better muscle strength recovery. Conclusion: NMES combined with standard physical therapy significantly enhances quadriceps muscle strength recovery after ACL surgery. Starting NMES treatment earlier in the post-operative period yields better muscle strength recovery. Citation: Li Z, Jin L, Chen Z, et al. Effects of Neuromuscular Electrical Stimulation on Quadriceps Femoris Muscle Strength and Knee Joint Function in Patients After ACL Surgery: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Orthop J Sports Med. 2025;13(1):23259671241275071. Published 2025 Jan 13. doi:10.1177/23259671241275071

Blog post
Immediate Pain Relief Effect of Low Level Laser Therapy for Sports Injuries: Randomized, Double-Blind Placebo Clinical TrialA. Takenori, M. Ikuhiro, U. Shogo, K. Hiroe, S. Junji, T. Yasutaka, K. Hiroya, N. Miki Published in: Journal of Science and Medicine in Sport, 2016 http://dx.doi.org/10.1016/j.jsams.2016.03.006 This clinical trial was conducted to determine whether laser therapy can give athletes with an orthopedic sports injury immediate pain relief. Thirty-two college athletes experiencing pain with motion after injury were randomized to receive one session of either laser therapy or placebo laser therapy. The study had no restriction on the location of the injury so laser therapy was used on multiple areas of the body in the study including foot, ankle, knee, back, elbow, and shoulder. Laser therapy group: These patients were treated for 10 minutes for a total energy dose of 108 J focused over the most painful area. Placebo group: These patients were treated for the same amount of time as the laser therapy group with the probe over the most painful area, but no power was emitted from the probe. Pain during motion was assessed for each patient before and after laser therapy using the Modified Numerical Rating Scale. Immediately after one treatment session, the laser therapy group pain scores were significantly better than those in the placebo group. The laser therapy group pain scores decreased by 36.94% while the placebo group pain scores only decreased by 8.2%. Study analysis demonstrated that significant immediate pain relief occurred in 75% of the athletes. The authors conclude that laser therapy is a useful modality for helping athletes get immediate pain relief.

Blog post
Utilizing Extracorporeal Shockwave Therapy for In-Season Athletes, an EditorialHye Chang Rhim, Joanne Borg-Stein, Steven Sampson, and Adam S. Tenforde Published in: Healthcare, 2023 https://doi.org/10.3390/healthcare11071006 Treatment methods that are able to give patients positive results within 3 months of injury are ideal for in-season athletes. The authors suggest that shockwave therapy may be one such method to quickly address sport-related muscle aches and pains and get athletes back in the game. Shockwave therapy uses the energy of sound waves to elicit biological effects at the cellular level which can then stimulate biochemical pathways involved in functions such as tissue repair and pain reduction. There are two types of shockwave therapy: Focus Shockwave Therapy and Radial Shockwave Therapy. With radial shockwave, the sound waves flow in an outward pattern and the energy stays closer to the surface. With focus shockwave, the sound waves converge allowing the energy to penetrate deeper into the body. There is a body of clinical evidence that demonstrates shockwave therapy can help to effectively treat sport-related musculoskeletal conditions such as plantar fasciitis, medial tibial stress syndrome, Achilles tendinopathy, and hamstring tendinopathy. Invasive therapies such as corticosteroid and platelet-rich plasma injections have also had positive results in treating athletes. However, these treatments can be linked to complications like infection and bleeding and tend to require long recovery times. Shockwave therapy, however, has a good safety profile, and athletes, depending on the condition, may be able to continue activity as tolerated. Based on current evidence in the field, the authors conclude that shockwave therapy may be used as part of the physical therapy program to help facilitate athletes returning to sport and keeping athletes from being sidelined for the season.

Blog post
Clinical Effectiveness of Multi-Wavelength Photobiomodulation Therapy as an Adjunct to Extracorporeal Shockwave Therapy in the Management of Plantar Fasciitis: A Randomized Controlled TrialMary Kamal Nassif Takla and Soheir Shethata Rezk-Allah Rezk Published in: Lasers in Medical Science, 2019 https://doi.org/10.1007/s10103-018-2632-4 This clinical trial evaluated the effectiveness of combining extracorporeal shockwave therapy (ESWT) with photobiomodulation therapy (PBMT) to treat pain and disability in patients with plantar fasciitis. One hundred twenty patients with plantar fasciitis for more than 6 months and unresponsive to conservative treatment were enrolled in the trial. Patients were randomized to one of the following groups: ESWT: Patients in this group were treated with the Chattanooga® Intelect® Focus Shockwave. Treatment sessions were completed once a week for 3 weeks and consisted of 2000 pulses at an energy level between 0.22 and 0.28 mJ/mm2. PBMT: Patients in this group received photobiomodulation therapy at a dose of 2.8 J/cm2 for 60 seconds at each session. Treatments were completed 3 times a week for 3 weeks. ESWT + PBMT: Treatment parameters for this group were the same as described for each of the single therapy groups. Patients received one ESWT and 3 PBMT treatments per week. Once per week, ESWT and PBMT were given consecutively with ESWT being administered prior to PBMT. Sham PBMT: Patients in this group received sham PBMT 3 times a week for 3 weeks where no power was emitted from the device. Study outcomes included pressure pain threshold (PPT), VAS pain score, and the functional foot index disability subscale (FFI-d). The ESWT, PBMT, and ESWT + PMBT groups showed improvement in all outcome scores after 3 weeks of treatment, with further improvement at the 12 week follow-up. The ESWT + PBMT group was superior to either treatment alone in reducing pain and disability. VAS pain scores for the ESWT + PBMT group decreased by 90.5% at the 12 week follow-up and the FFI-d scores decreased by 56.2%! In comparison, the Sham PBMT group VAS pain scores increased by 3.8% and the FFI-d scores increased by 0.6%. The authors concluded that both ESWT and PBMT are effective treatments for reducing pain and improving function in patients with plantar fasciitis. However, combining the two treatments gives the best results.

Blog post
How to Prepare Patients for Their First Photobiomodulation Therapy SessionAs a clinician offering photobiomodulation therapy (PBMT), helping your patients feel informed and at ease is key to long-term compliance and better outcomes. This guide is designed to help you walk first-time patients through what to expect during their initial PBMT session using LightForce® therapy lasers—so you can improve confidence and set realistic expectations from the start. The Basics: What Patients Should Know PBMT, in the case of LightForce therapy lasers, is a non-invasive therapy that uses near-infrared laser light to stimulate cellular activity, increase blood flow, and promote tissue repair. During the treatment session: The laser is applied directly to the treatment area. Sessions last around 5–15 minutes depending on the condition. Patients may feel gentle warmth, tingling, or no sensation at all. Most return to normal activity immediately. Preparing Patients Before Their Session Patients don’t need to make special preparations, but you can advise the following: Wear loose, comfortable clothing that allows access to the treatment area. Discuss any medications, implants, or sensitivities before starting therapy. Image Step-by-Step: What a Standard Session Looks Like Here’s how to walk patients through the PBMT process: 1. Clinical Evaluation & Protocol Setup You’ll begin with a brief assessment, reviewing: The patient’s condition Medical history Treatment goals Based on these factors, select the appropriate LightForce® laser built-in protocol or use the Perfect Protocol software to select your own treatment parameters. 2. Positioning the Patient Position the patient seated or lying down to ensure comfort and proper exposure to the affected area. 3. Laser Application Use the LightForce® therapy laser to deliver precise energy to the target tissues. Depending on the treatment head in use, glide or hover the applicator head over the skin with controlled movement. Follow the Empower IQ™ technology to ensure you are treating effectively. Monitor patient feedback. 4. Session Duration Most treatments take 5–15 minutes depending on area size and number of treatment sites. 5. Sensory Feedback Many patients report: A soothing warmth Slight tingling Occasionally, no noticeable sensation Image Aftercare and Clinical Notes PBMT requires no downtime. Patients can return to daily activity. According to clinical literature and provider experience: PBMT is well-tolerated with few reported side effects. Clinicians report that 91% of patients have a clinically meaningful reduction in pain after laser treatments.¹ Results Timeline: What to Tell Your Patients Acute or mild conditions: improvement may be felt after 1–3 sessions. Chronic or complex cases: typically require 6–12 sessions or more. Initial frequency: 2–3 sessions per week is standard to jumpstart results. Common Patient FAQs (and How to Answer Them) Does PBMT hurt? No. The treatment is non-invasive and well-tolerated, with most patients reporting mild warmth or tingling. Can it be used with other treatments? Yes. PBMT is often combined with physical therapy, chiropractic adjustments, rehab programs, and other modalities such as shockwave therapy. Is it covered by insurance? Not usually. Many practices like ours offer affordable out-of-pocket options. Why LightForce® Makes a Difference for Providers LightForce® therapy lasers are engineered with advanced controls to support safety, comfort, and outcomes for providers and patients alike. Key features include: Built-in protocols for specific conditions Perfect Protocol software to allow the clinician to select treatment parameters Visual guidance and treatment monitoring with the Empower IQ technology Reliable power delivery for consistent results FDA-cleared systems trusted by top health organizations and sports teams Image Help Patients Feel Confident from Day One When you clearly communicate what to expect, you not only help set realistic expectations—you build trust. LightForce® makes this easier with: Provider training and onboarding support Built-in clinical protocols Marketing tools to help educate patients Schedule a demo to learn how LightForce® therapy lasers can help elevate your clinical outcomes. Sources: 1. Enovis (2023). Post-Market Clinical Follow-Up Retrospective Study Report: LightForce® Therapy Lasers. Internal Enovis report. Unpublished.